If someone near you has sudden, severe tearing chest or back pain — call emergency services immediately and do not drive. Aortic dissection is one of the few conditions where minutes determine survival.
Aortic dissection is a tear in the inner wall of the aorta that allows blood to surge between the layers of the aortic wall — and it is the most time-critical emergency in cardiac surgery. Unlike most cardiac conditions, aortic dissection symptoms have a characteristic that distinguishes them from almost everything else: the pain is at its absolute worst the moment it begins. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, explains aortic dissection symptoms, the classification that determines treatment urgency, and what family members need to know when every minute counts.
What Is Aortic Dissection?
The aortic wall has three layers. In aortic dissection, the innermost layer (intima) develops a tear — and blood under arterial pressure forces through that tear and strips the layers apart along the length of the aorta, creating a false channel (false lumen) alongside the true blood channel.
As this false channel extends, it can compress the true channel — cutting off blood supply to organs. It can propagate backwards toward the heart — causing severe aortic regurgitation or cardiac tamponade. It can block the openings of coronary arteries — causing a simultaneous heart attack. And it can rupture through the outer wall — causing catastrophic internal haemorrhage. This cascade can progress from tear to death in under an hour in the worst cases.
Aortic Dissection Symptoms — The Defining Characteristics
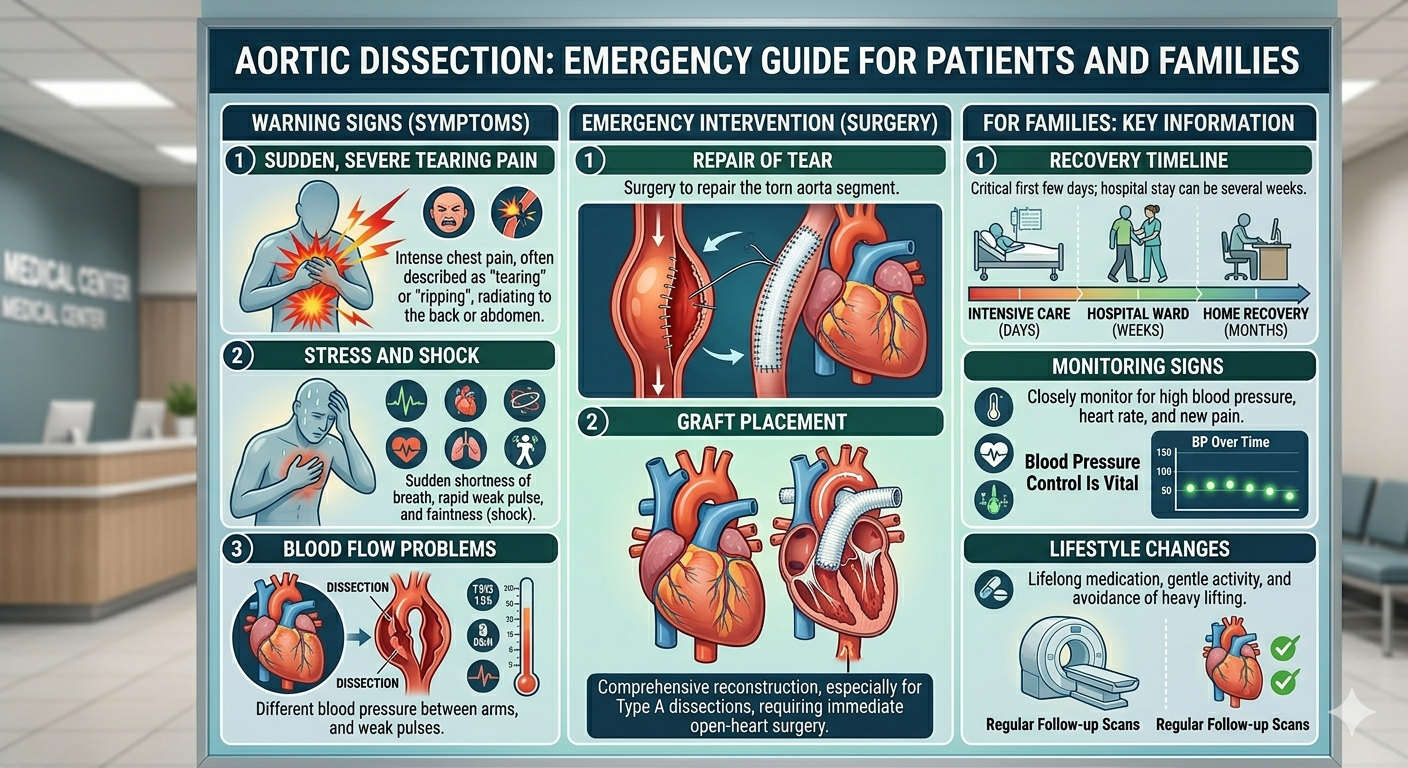
Tearing or Ripping Chest or Back Pain — Maximum at Onset
This is the single most important aortic dissection symptom, and what separates it clinically from almost every other cardiac emergency. Patients describe it as tearing, ripping, or like something exploding inside the chest. It is at maximum intensity from the very first second — not building gradually. Most patients describe it as the worst pain they have ever experienced in their life. It often radiates to the back, between the shoulder blades.
Migrating Pain
As the dissection extends down the aorta, the pain follows it — moving from the chest to the back, then toward the abdomen. Migrating pain is highly specific for aortic dissection and should always trigger immediate emergency assessment with CT angiography.
Blood Pressure Difference Between the Two Arms
A systolic blood pressure difference of more than 20 mmHg between the right and left arm — caused by the dissection narrowing or blocking the artery to one arm — is a clinical sign strongly associated with aortic dissection. In emergency settings, blood pressure should always be measured in both arms when dissection is suspected.
Neurological Symptoms
Sudden weakness, numbness, or paralysis of an arm or leg — caused by the dissection compromising blood supply to the spinal cord or carotid arteries. When aortic dissection presents with stroke symptoms, it is particularly dangerous because thrombolytic drugs (clot-busters given in stroke) are absolutely contraindicated — they would cause fatal haemorrhage in a dissection.
Absent Pulse in One Limb
If the dissection extends into a major branch artery, the pulse may disappear in one arm or leg.
Stanford Classification — Type A vs Type B
The most important classification in aortic dissection. Everything — urgency, treatment, mortality — hinges on which type it is.
Type A — Surgical Emergency
Any dissection involving the ascending aorta (the section of aorta rising from the heart) — regardless of where the original tear is. Mortality is approximately 1–2% per hour without surgery. Emergency surgical replacement of the ascending aorta must be performed as soon as the operating team can be assembled — ideally within 2 hours of diagnosis. This is one of the most technically demanding emergency operations in cardiac surgery.
Type B — Medical Management Initially
Dissection involving only the descending aorta, below the left subclavian artery, not extending into the ascending aorta. Uncomplicated Type B is managed medically — strict blood pressure and heart rate control in a cardiac ICU with IV medications. Complicated Type B — with evidence of organ malperfusion, rapidly expanding false lumen, or threatened rupture — requires urgent endovascular repair (TEVAR).
What to Tell the Emergency Room Team
If you suspect aortic dissection in yourself or a family member, say these specific words to the emergency team:
- “Sudden, severe chest or back pain that was worst immediately when it started”
- “The pain feels like tearing or ripping”
- “They have high blood pressure” (or Marfan syndrome, or a known aortic aneurysm, if applicable)
This prompts immediate CT aortic angiography — the definitive test that confirms or excludes aortic dissection within minutes. Do not let the team assume heart attack and give thrombolytics without a CT scan — in aortic dissection, this would be fatal.
Risk Factors for Aortic Dissection
- Hypertension — the most common risk factor. Poorly controlled blood pressure progressively weakens the aortic wall.
- Marfan syndrome — inherently weak aortic wall; dissection can occur at younger ages and smaller aortic diameters.
- Bicuspid aortic valve — associated with ascending aortic enlargement and dissection risk.
- Existing aortic aneurysm — an enlarged aorta is at higher risk of dissection; learn more about aortic aneurysm.
- Pregnancy — third trimester and peripartum period; rare but important cause of Type A dissection in young women.
Emergency Surgery for Type A Aortic Dissection
The operation is performed under general anaesthesia on cardiopulmonary bypass. The ascending aorta is replaced with a synthetic Dacron graft. If the dissection extends into the aortic arch, deep hypothermic circulatory arrest — cooling the body to 18°C and temporarily stopping circulation — allows the surgeon to repair the arch safely. If the aortic valve root is involved, it may be repaired or replaced simultaneously. Total operating time: 4–8 hours. This is among the highest-stakes operations in all of surgery — and one that Dr. Ved Prakash performs as part of the aortic surgery programme at Yatharth Hospital.
Frequently Asked Questions — Aortic Dissection Symptoms Emergency
What are the symptoms of aortic dissection?
Sudden, severe tearing or ripping chest or back pain at maximum intensity from the first moment. Often with migrating pain as the dissection extends, a blood pressure difference between the two arms, and sometimes neurological symptoms. Any combination of these requires immediate emergency CT angiography.
What is the difference between Type A and Type B aortic dissection?
Type A involves the ascending aorta — emergency surgery required, mortality rises 1–2% per hour. Type B involves only the descending aorta — managed with blood pressure control initially, with TEVAR for complications.
How is aortic dissection different from a heart attack?
Dissection pain is worst at the very first second and described as tearing. Heart attack pain builds gradually and is described as pressure. Both are emergencies — CT angiography distinguishes them rapidly and changes the entire treatment plan.
Can aortic dissection be survived?
Yes — with emergency surgery for Type A, many patients survive and return to near-normal life. Mortality at experienced centres is 15–25% with emergency surgery — compared to near-certain death without it. Long-term survivors need lifelong blood pressure control and regular aortic imaging.
Dr. Ved Prakash | Director, CTVS — Yatharth Super Speciality Hospitals, Greater Noida
📞 +91-9355255106 |
📧 drvedprakash@gmail.com |
Book Appointment →