When a mitral valve is diseased enough to require surgery, the first question every patient should ask is not “when do I have the operation” — it is “can my valve be repaired rather than replaced?” Mitral valve repair and mitral valve replacement are not equivalent options. Repair is significantly better when it is feasible — better survival, better heart muscle preservation, and no need for lifelong blood thinners. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, explains how the repair vs replacement decision is made and what it means for your life after surgery.
Why Repair Is Always Preferred When Feasible
The mitral valve is not just a mechanical flap. It is a complex functional unit — the two leaflets, the annulus (fibrous ring), the chordae tendineae (tendon-like cords), and the papillary muscles (muscle pillars inside the ventricle) all work together to ensure the valve opens fully and closes completely with each heartbeat. When this apparatus is preserved through repair, the left ventricle continues to function in its normal geometry. When it is replaced, the relationship between the valve and the ventricular muscle is altered — and long-term left ventricular function is slightly worse after replacement than after repair, even with the best prosthetic valves.
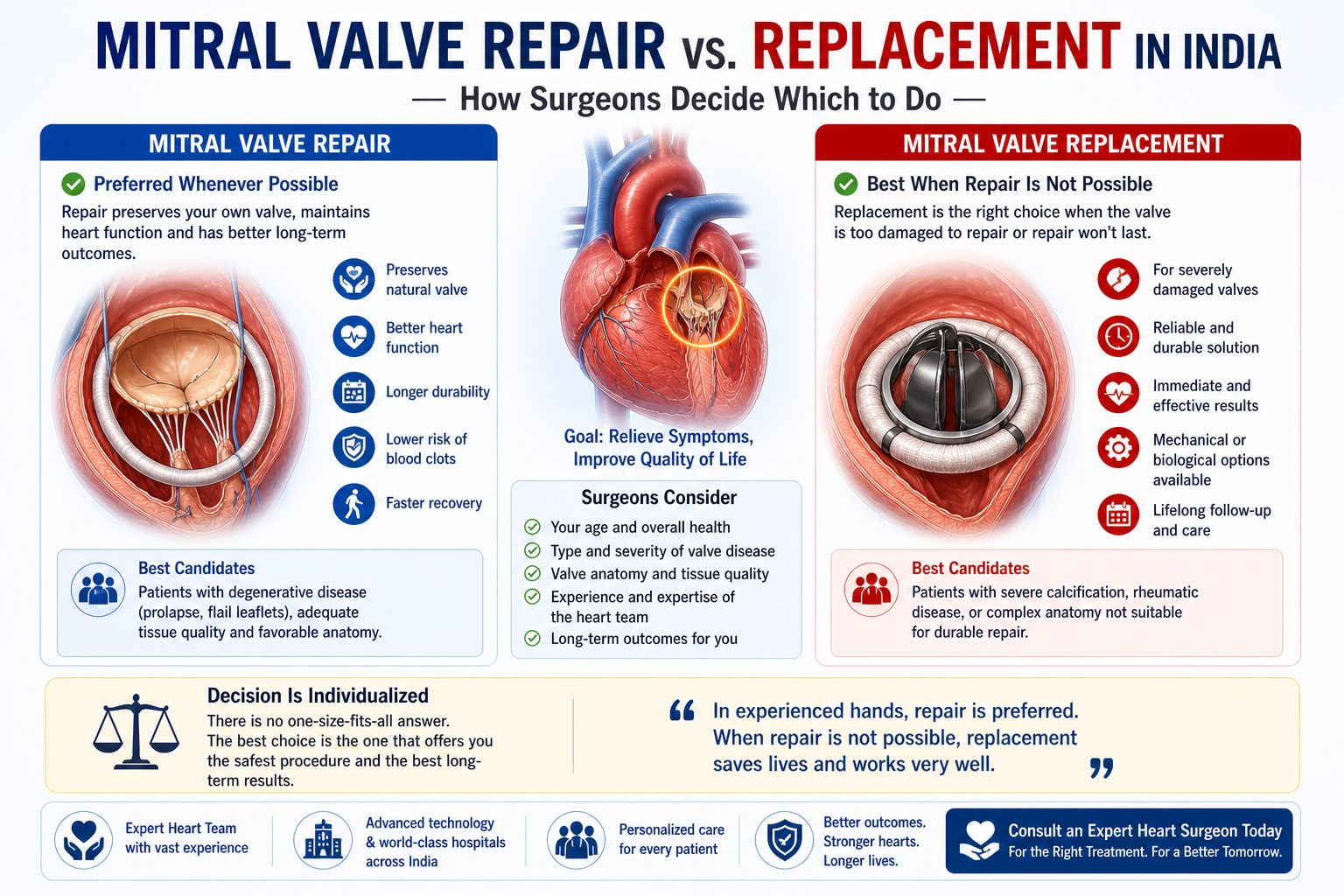
The specific advantages of mitral valve repair over replacement:
- No prosthetic valve: No risk of prosthetic valve endocarditis (infection), no valve thrombosis risk, no structural valve deterioration over time
- No lifelong warfarin: After repair, anticoagulation is typically only needed for 3 months — then stopped entirely (unless atrial fibrillation is also present)
- Better left ventricular function: The subvalvular apparatus is preserved — which maintains the geometric relationship between the valve and the heart muscle
- Better long-term survival: Multiple large studies show superior 10 and 20-year survival after repair compared to replacement in patients with degenerative mitral regurgitation
- No future valve replacement needed: A successful, durable repair is lifelong — no biological valve deterioration or need for a second operation in most patients
What Determines Whether Repair Is Possible — The Anatomy
The feasibility of mitral valve repair depends entirely on the anatomy of the diseased valve. Two factors matter most:
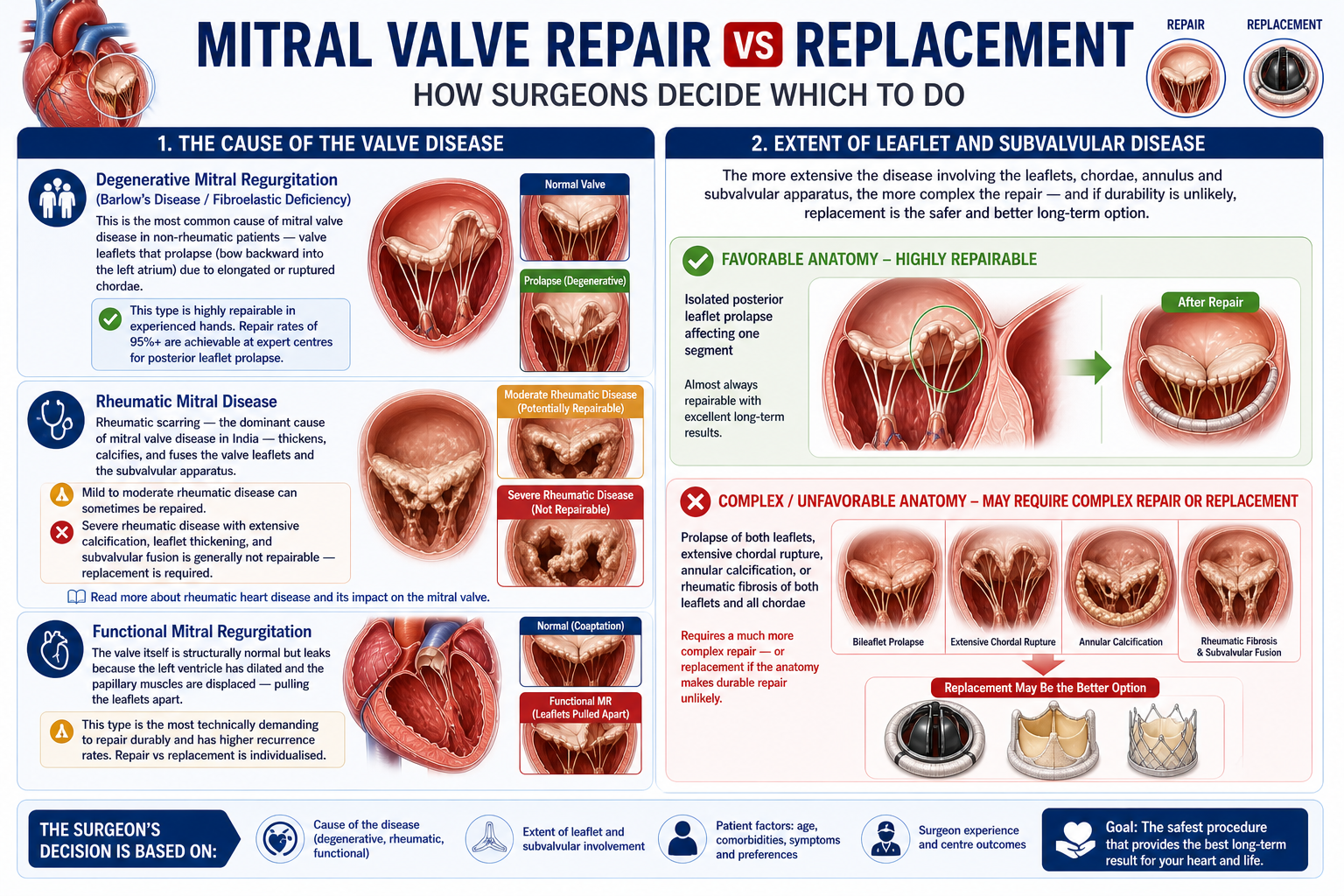
1. The Cause of the Valve Disease
Degenerative mitral regurgitation (Barlow’s disease / fibroelastic deficiency): This is the most common cause of mitral valve disease in non-rheumatic patients — valve leaflets that prolapse (bow backward into the left atrium) due to elongated or ruptured chordae. This type is highly repairable in experienced hands. Repair rates of 95%+ are achievable at expert centres for posterior leaflet prolapse.
Rheumatic mitral disease: Rheumatic scarring — the dominant cause of mitral valve disease in India — thickens, calcifies, and fuses the valve leaflets and the subvalvular apparatus. Mild to moderate rheumatic disease can sometimes be repaired. Severe rheumatic disease with extensive calcification, leaflet thickening, and subvalvular fusion is generally not repairable — replacement is required. Read more about rheumatic heart disease and its impact on the mitral valve.
Functional mitral regurgitation: The valve itself is structurally normal but leaks because the left ventricle has dilated and the papillary muscles are displaced — pulling the leaflets apart. This type is the most technically demanding to repair durably and has higher recurrence rates. Repair vs replacement is individualised.
2. Extent of Leaflet and Subvalvular Disease
A valve with isolated posterior leaflet prolapse affecting one segment is almost always repairable. A valve with prolapse of both leaflets, extensive chordal rupture, annular calcification, or rheumatic fibrosis of both leaflets and all chordae requires a much more complex repair — or replacement if the anatomy makes durable repair unlikely.
The Repair Techniques Used
Mitral valve repair is not a single operation — it is a set of techniques tailored to the specific anatomy:
- Resection and repair of prolapsing segments: The prolapsing portion of leaflet is excised and the remaining tissue is re-approximated — the most common technique for posterior leaflet prolapse
- Artificial chordae (ePTFE neo-chordae): New synthetic chords are attached from the papillary muscle to the leaflet edge, replacing ruptured native chordae — allows leaflet mobility to be restored without resection
- Commissurotomy: For rheumatic mitral stenosis with fused commissures — the fused edges are surgically split to widen the valve opening
- Annuloplasty ring: A shaped ring is sewn around the valve annulus — in virtually all repairs — to reduce the annulus to normal size, support the repair, and prevent recurrence of regurgitation
What Mitral Valve Replacement Means — and When It Is the Right Choice
When repair is not feasible, replacement is performed. The diseased valve is removed and a prosthetic valve — either mechanical or biological tissue — is sewn in its place.
- Mechanical valve: Lasts indefinitely but requires lifelong warfarin (INR 2.5–3.5 for mitral position). Standard choice in younger patients (under 60–65) with rheumatic heart disease in India — where reliability and durability over decades outweigh the inconvenience of anticoagulation.
- Biological tissue valve: Does not require lifelong warfarin after the initial 3 months. However, biological valves in the mitral position have a shorter lifespan in younger patients — typically 12–15 years before structural deterioration. More appropriate for elderly patients or those in whom anticoagulation is contraindicated.
The Most Important Question to Ask Your Surgeon
Before any mitral valve surgery, ask your cardiac surgeon directly: “Have you assessed whether my valve can be repaired? What is your personal repair rate for my type of valve disease?”
This matters because mitral valve repair requires significantly more surgical skill and experience than replacement — and not every cardiac surgeon has high repair rates. If you are told replacement is necessary without a clear explanation of why repair was not attempted or not feasible, you are entitled to seek a second surgical opinion.
For all types of heart valve surgery in Delhi NCR, including mitral valve repair and replacement, consult Dr. Ved Prakash at Yatharth Hospital, Greater Noida. Share your echocardiogram via WhatsApp at +91-9355255106 for a pre-assessment of repair feasibility before your visit.
Frequently Asked Questions — Mitral Valve Repair vs Replacement India
Is mitral valve repair better than replacement?
Yes — when feasible and durable, repair is superior to replacement. Better long-term survival, better heart muscle preservation, no need for lifelong warfarin, no prosthetic valve complications. Every patient should ask whether repair is possible before accepting replacement.
Can all mitral valves be repaired?
No. Extensive rheumatic calcification, bilateral leaflet disease, and severe subvalvular fusion typically cannot be repaired durably. Degenerative mitral regurgitation (leaflet prolapse) is highly repairable in expert hands — repair rates of 95%+ for posterior leaflet prolapse.
Do I need warfarin after mitral valve surgery?
After repair — 3 months only, then stopped (unless atrial fibrillation is present). After mechanical replacement — lifelong warfarin. After biological tissue replacement — 3 months only, then stopped.
What is the success rate of mitral valve repair?
Freedom from reoperation at 10 years exceeds 90–95% for degenerative regurgitation at expert centres. Surgeon volume is the strongest predictor — ask how many repairs your surgeon performs annually.
Dr. Ved Prakash | Director, CTVS — Yatharth Super Speciality Hospitals, Greater Noida
📞 +91-9355255106 |
📧 drvedprakash@gmail.com |
Book Appointment →
