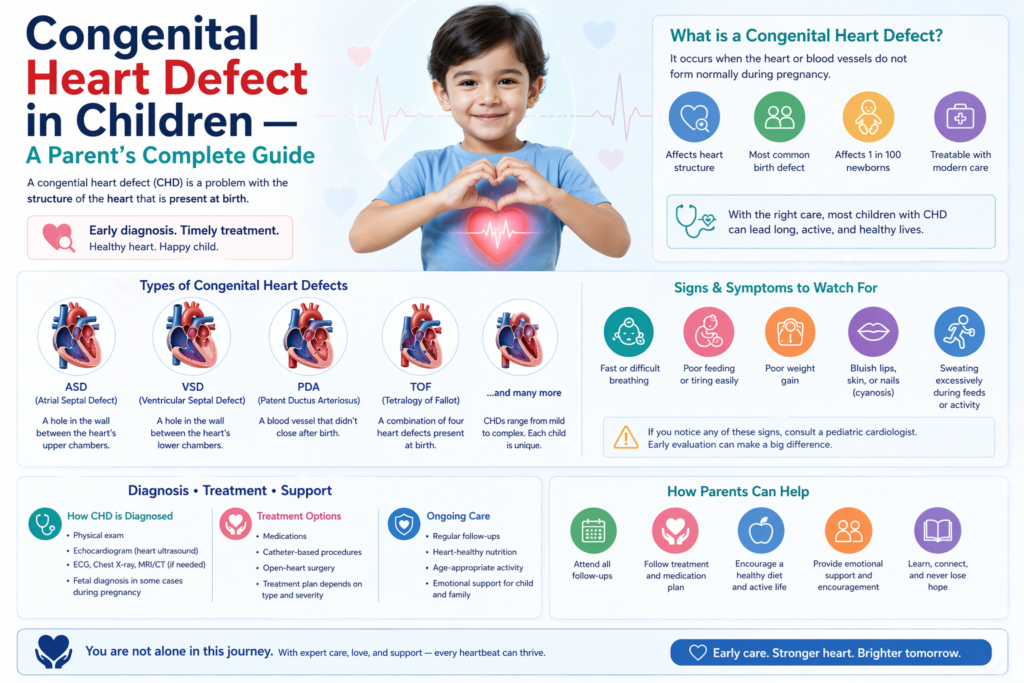
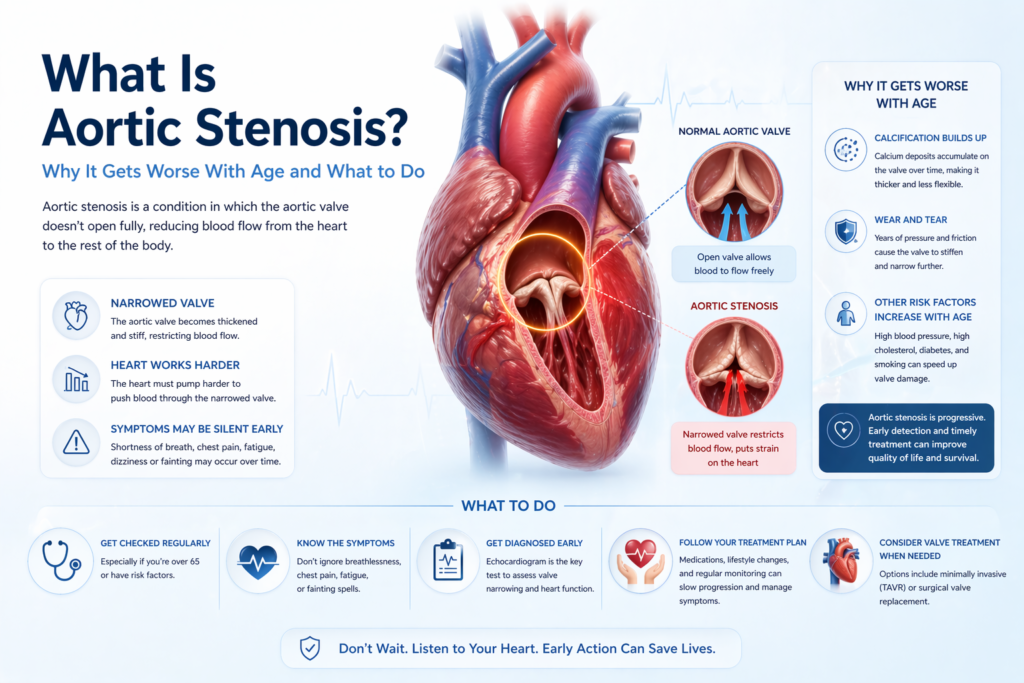
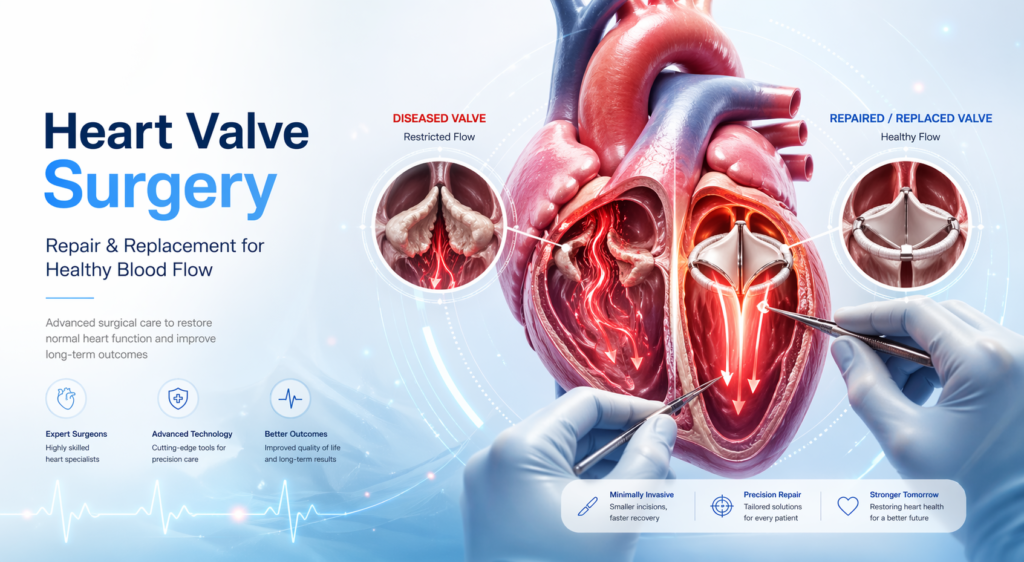
For heart surgery, Dehradun patients have traditionally needed to travel to AIIMS Rishikesh, Delhi, or Chandigarh — journeys of 5–7 hours that are stressful for cardiac patients and costly for families. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida — approximately 4 hours from Dehradun via NH-334 and NH-58 — provides full-service cardiac surgery for Dehradun and Uttarakhand patients with the quality of Delhi’s best hospitals and significantly more accessible costs. Why Dehradun Patients Choose Yatharth Hospital for Heart Surgery Dehradun’s cardiac facilities are limited to cardiology — coronary angiography, angioplasty, and pacemaker implantation are available. But bypass surgery, valve repair and replacement, aortic surgery, and paediatric heart surgery for Dehradun patients require travel. The options are: AIIMS Rishikesh: Excellent institution but long waiting lists for elective CTVS surgery — often 6–12 weeks for non-emergency cases Delhi (AIIMS, Apollo, Max, Fortis): 5–6 hours from Dehradun by road — feasible but exhausting for cardiac patients Yatharth Hospital, Greater Noida: 3.5–4 hours from Dehradun via NH-334/NH-58 — closer than central Delhi, with shorter waiting times and more accessible costs Chandigarh (PGI, Fortis Mohali): 5 hours from Dehradun What Heart Surgery Is Available for Dehradun Patients at Yatharth Hospital? Bypass surgery (CABG): For Dehradun patients referred after angiography — on-pump and off-pump bypass surgery available. No waiting list for referred urgent cases. Mitral and aortic valve surgery: Repair and replacement for rheumatic and degenerative valve disease — significant in the Uttarakhand hill district population TAVI: For elderly Dehradun patients with aortic stenosis too frail for open surgery — available without the journey to AIIMS Delhi Paediatric heart surgery: ASD, VSD, TOF repair for children from Dehradun and Uttarakhand Aortic aneurysm and EVAR/TEVAR Varicose vein laser treatment (EVLT) Getting Started From Dehradun WhatsApp pre-assessment: Send angiogram/echo/CT report to +91-9355255106. Dr. Ved Prakash reviews and advises on urgency, surgical plan, and cost estimate before travel. Online consultation: Available for initial assessment without travel — particularly useful for Dehradun patients to determine urgency before committing to the journey. Insurance: Ayushman Bharat PM-JAY, CGHS, ECHS, and major insurance accepted. Uttarakhand state government health scheme patients should confirm empanelment before visiting. Frequently Asked Questions — Heart Surgery Dehradun How far is Yatharth Hospital from Dehradun? Yatharth Super Speciality Hospitals, Greater Noida is approximately 280–300 km from Dehradun via NH-334 (Haridwar) and NH-58 — a drive of 3.5–4 hours. The route is well maintained and manageable for a family travelling with a cardiac patient. Is bypass surgery available near Dehradun? Full-service CTVS (bypass surgery, valve surgery, aortic surgery) is not available in Dehradun city as of 2026. The nearest cardiac surgery centres are Yatharth Hospital Greater Noida (3.5–4 hours), AIIMS Rishikesh (35 minutes but long waiting lists), and hospitals in Delhi (5–6 hours). Can I get a second opinion for heart surgery from Dehradun without travelling? Yes — Dr. Ved Prakash provides online cardiac second opinion consultations for Dehradun patients. Share your angiogram, echocardiogram, and any clinical reports via WhatsApp at +91-9355255106. A video consultation is arranged and a full clinical opinion is provided before you travel for surgery. Dr. Ved Prakash | Director CTVS — Yatharth Super Speciality Hospitals, Greater Noida 📞 +91-9355255106 | Book Appointment → Tetralogy of Fallot — TOF — is the most common cyanotic congenital heart defect, and tetralogy of Fallot symptoms include the bluish colouration of the skin (cyanosis) that gives this condition its most well-known description: the “blue baby.” With timely surgery, children with tetralogy of Fallot grow up to live full, active lives — but the journey from diagnosis to long-term follow-up requires parents to be well informed. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, explains tetralogy of Fallot symptoms, what surgery involves, and what long-term care is needed. What Is Tetralogy of Fallot? Tetralogy of Fallot is a combination of four structural heart defects present from birth: A large VSD (Ventricular Septal Defect) — a large hole between the two lower heart chambers Pulmonary stenosis — narrowing of the outflow from the right ventricle to the pulmonary artery (the vessel taking blood to the lungs), sometimes involving the pulmonary valve itself Overriding aorta — the aorta is positioned directly over the VSD, receiving blue (deoxygenated) blood from the right ventricle as well as oxygenated blood from the left Right ventricular hypertrophy — the right ventricle thickens because it is working against the obstructed pulmonary outflow The combination of these four defects means that oxygen-depleted blood bypasses the lungs and is pumped to the body through the aorta — causing the characteristic cyanosis (blue discolouration) that defines tetralogy of Fallot symptoms. Tetralogy of Fallot Symptoms — What Parents Notice Cyanosis (bluish skin): The most characteristic tetralogy of Fallot symptom — blue or purple discolouration of the lips, tongue, fingernails, and toenails. Cyanosis may be present at birth or appear in the first weeks of life as the ductus arteriosus (a fetal blood vessel) closes. “Tet spells” — hypercyanotic episodes: Episodes of sudden, intense cyanosis — the baby turns very blue, becomes irritable or inconsolable, breathes very fast, and may briefly lose consciousness. Tet spells are caused by spasm of the right ventricular outflow tract that suddenly reduces blood flow to the lungs. They are a medical emergency. Squatting in older children: Older children with unrepaired TOF instinctively squat after physical activity — squatting increases systemic vascular resistance and reduces the right-to-left shunting, providing temporary symptom relief Poor growth and feeding difficulties in untreated infants Exercise intolerance in older children with partial defects Clubbing of fingers and toes — in children with long-standing cyanosis How Is Tetralogy of Fallot Diagnosed? Foetal echocardiogram: TOF can often be detected at the 18–20 week anomaly scan — allowing planned delivery at a centre with paediatric cardiac surgery Neonatal echocardiogram: Confirms the diagnosis and anatomical details after birth Pulse oximetry screening: Low oxygen saturation detected at birth routine screening CT cardiac angiography: For detailed assessment of the pulmonary artery anatomy before surgical