An aortic aneurysm is a bulge or ballooning in the wall of the aorta — the body’s main artery — and it is one of the most dangerous conditions in medicine because an aortic aneurysm typically causes no symptoms until it is on the verge of rupturing. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, explains what is an aortic aneurysm, when it becomes dangerous, how it is diagnosed, and what surgery involves.
What Is an Aortic Aneurysm?
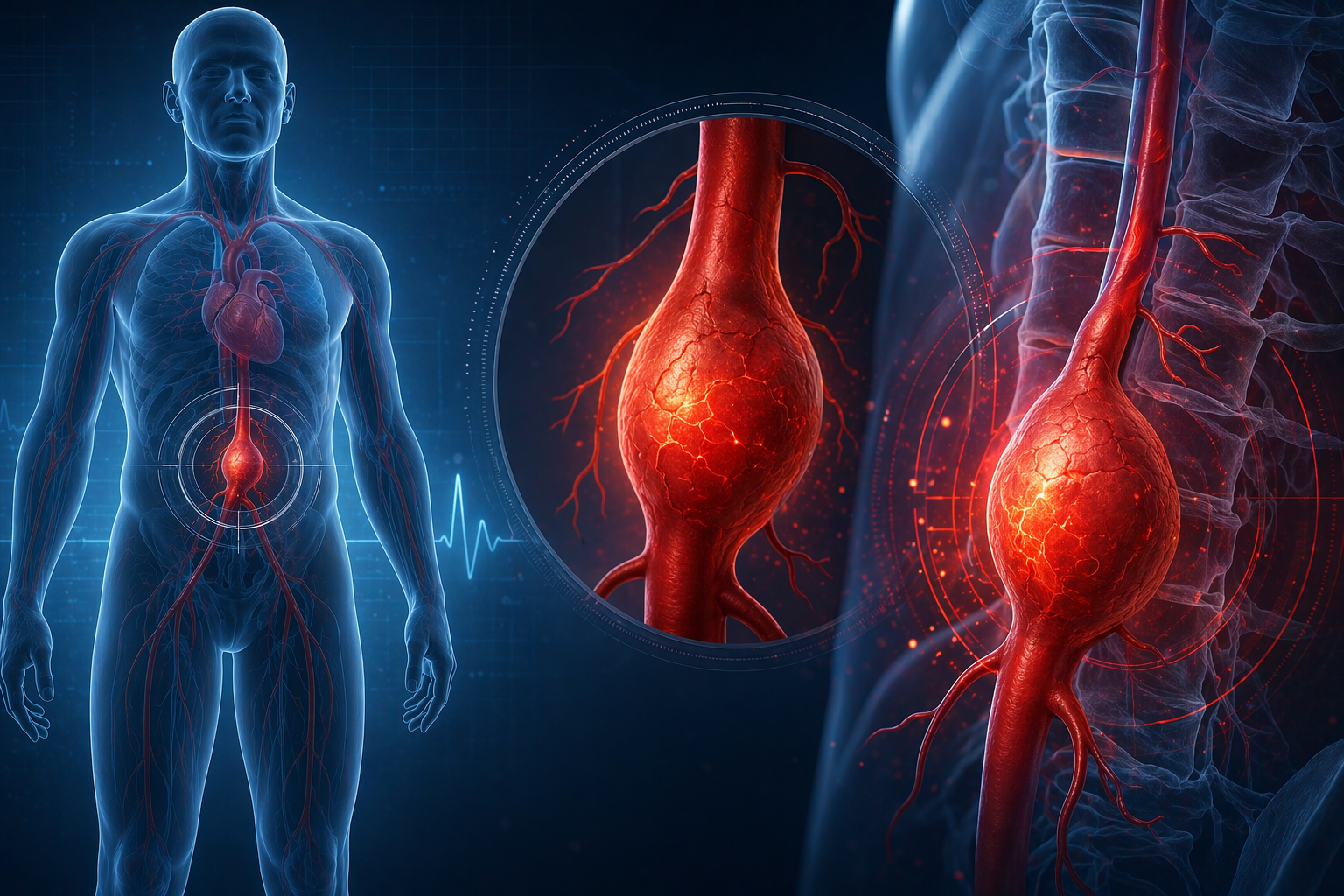
The aorta is the largest artery in the body — rising from the heart, arching through the chest, and running down through the abdomen to supply the entire body. The normal aortic diameter is approximately 2.5–3.0 cm. An aortic aneurysm is an abnormal widening of the aorta to more than 1.5 times its normal diameter — typically defined as greater than 3.0 cm in the abdominal aorta or greater than 4.5 cm in the thoracic (chest) aorta.
As an aortic aneurysm enlarges, the wall of the aorta becomes progressively thinner and weaker. At a critical size, the wall can rupture — releasing enormous volumes of blood into the chest or abdomen. Rupture of an aortic aneurysm carries a mortality rate exceeding 80% even with emergency surgery. This is why detecting and treating an aortic aneurysm before rupture is so critical.
Types of Aortic Aneurysm
Abdominal Aortic Aneurysm (AAA)
An aortic aneurysm in the portion of the aorta that runs through the abdomen — the most common location. AAAs occur primarily in men over 65 with a history of smoking, hypertension, or a family history of aortic aneurysm. They are frequently detected incidentally on ultrasound or CT scan performed for another reason — because they rarely cause symptoms until they are very large or rupturing.
Thoracic Aortic Aneurysm (TAA)
An aortic aneurysm in the aorta within the chest — either the ascending aorta (rising from the heart), the arch (the curved section at the top), or the descending aorta (running down behind the heart). TAAs are more often associated with genetic conditions (Marfan syndrome, bicuspid aortic valve) and hypertension, and can occur at younger ages than AAAs.
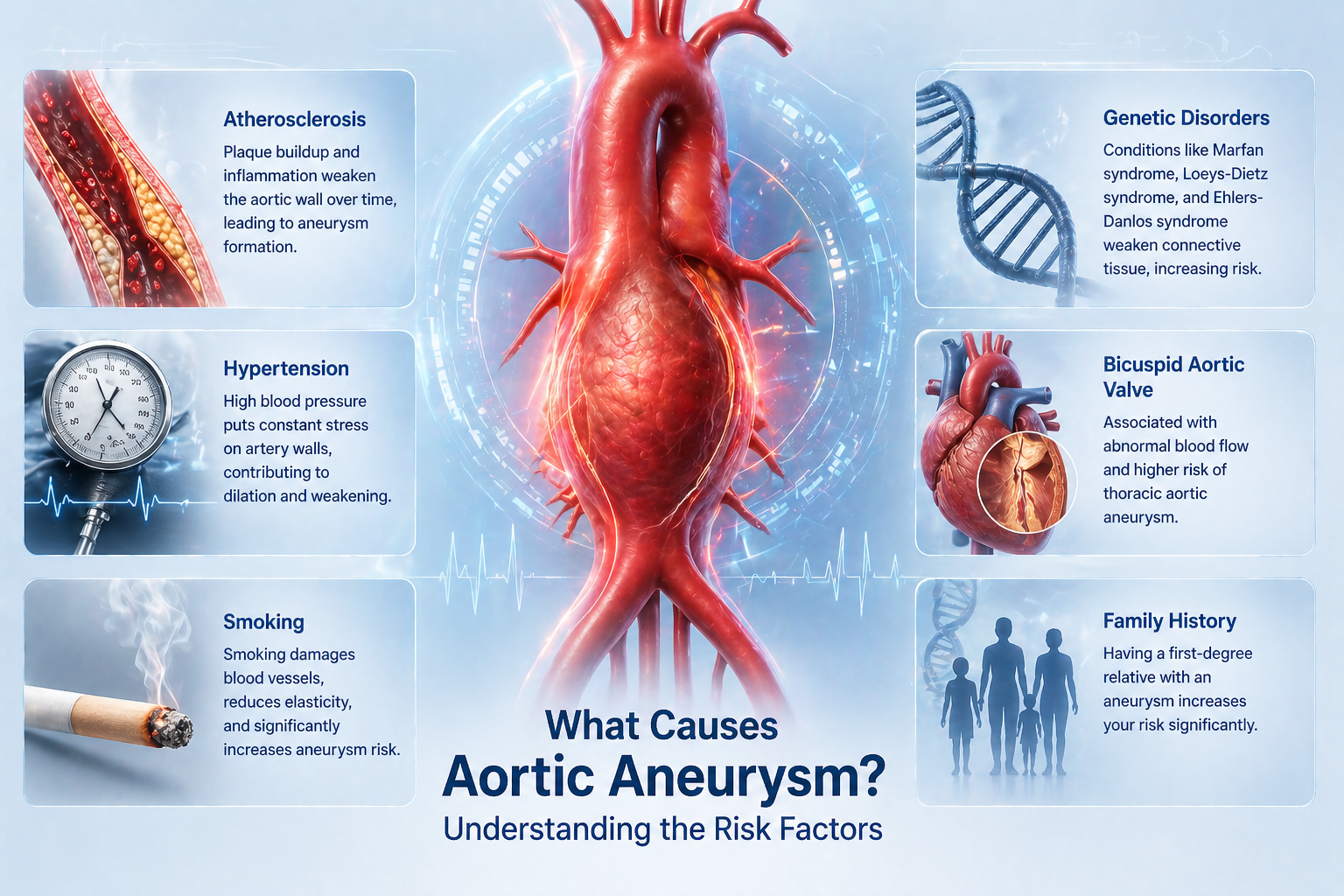
What Causes an Aortic Aneurysm?
- Atherosclerosis: The primary cause of AAA — decades of high blood pressure, high cholesterol, and smoking cause the aortic wall to degenerate
- Hypertension: The most important modifiable risk factor — controlling blood pressure slows aortic aneurysm growth
- Smoking: Doubles aortic aneurysm risk and accelerates growth rate significantly
- Genetic connective tissue disorders: Marfan syndrome, Loeys-Dietz syndrome, and Ehlers-Danlos syndrome predispose to thoracic aortic aneurysms — often at young ages
- Bicuspid aortic valve: Associated with progressive thoracic aortic aneurysm — regular aortic surveillance with echocardiogram or CT is essential
- Family history: First-degree relatives of AAA patients have a 10–15% lifetime risk — screening ultrasound is recommended
Aortic Aneurysm Symptoms — Why It Is Called the Silent Killer
The vast majority of aortic aneurysms are completely asymptomatic until rupture or acute expansion. When symptoms do occur, they are usually:
- Deep, constant back or abdominal pain — particularly in the lower back, which may be confused with musculoskeletal pain. This is often a sign of a rapidly expanding or leaking AAA — a surgical emergency.
- Pulsating sensation in the abdomen — a pulsatile mass felt in the centre of the abdomen, like a second heartbeat. Most often felt by the patient themselves or detected on examination.
- Chest or back pain in thoracic aneurysm — from pressure on surrounding structures. A descending thoracic aneurysm may cause hoarseness (from recurrent laryngeal nerve compression) or difficulty swallowing.
- Rupture: Sudden, severe abdominal or back pain, collapse, and circulatory shock. A ruptured aortic aneurysm is the surgical emergency that every vascular surgeon dreads — and that mortality figures make sobering reading.
When Does an Aortic Aneurysm Need Surgery?
The treatment decision for an aortic aneurysm is based primarily on size — because larger aneurysms carry a significantly higher annual rupture risk:
| AAA Diameter | Annual Rupture Risk | Recommendation |
| 3.0–4.4 cm | <0.5% | Surveillance ultrasound every 12 months |
| 4.5–5.0 cm | 1–3% | Surveillance every 6 months + surgical review |
| 5.0–5.5 cm | 5–10% | Surgery recommended for most patients |
| Over 5.5 cm | 10–25% | Surgery urgently recommended |
| Any size — rapidly expanding (>1cm/year) | High | Surgery recommended regardless of size |
Aortic Aneurysm Treatment — EVAR vs Open Surgery
- EVAR (Endovascular Aneurysm Repair): A stent-graft is delivered through the femoral arteries in the groin and positioned inside the aneurysm — excluding it from the circulation without opening the abdomen. Recovery is significantly faster (2–3 days hospital stay) and surgical risk is lower. Suitable for most infrarenal AAAs with suitable anatomy.
- Open surgical repair: The aneurysm is exposed through an abdominal incision, clamped, and replaced with a synthetic (Dacron) graft. More invasive — 7–10 day hospital stay — but the definitive lifelong repair. Required when the anatomy is not suitable for EVAR, or for juxtarenal/suprarenal aneurysms.
- TEVAR (Thoracic Endovascular Aortic Repair): The endovascular equivalent of EVAR for descending thoracic aortic aneurysms — a stent-graft deployed through the femoral artery to reline the thoracic aorta.
Frequently Asked Questions — What Is Aortic Aneurysm
What is an aortic aneurysm and is it always fatal?
An aortic aneurysm is an abnormal bulging of the aorta. It is not immediately fatal — most detected aneurysms are small, grow slowly, and are treated safely with elective surgery before they rupture. A ruptured aortic aneurysm, however, carries a mortality rate exceeding 80%. Early detection and timely elective repair are what save lives.
How is an aortic aneurysm found if there are no symptoms?
Most aortic aneurysms are discovered incidentally — on an ultrasound for kidney or liver problems, or on a CT scan. Screening ultrasound is recommended for all men over 65 with a history of smoking, and for first-degree relatives of AAA patients.
Can an aortic aneurysm be treated without surgery?
Small aneurysms under 5 cm are managed with surveillance (regular size monitoring), blood pressure control, statin therapy, and smoking cessation — which slow growth. No medication reduces the aneurysm or reverses the wall damage. Surgery or EVAR is required once the size threshold is reached.
What is the recovery after EVAR surgery?
EVAR patients are typically discharged in 2–3 days and return to full activity within 2–4 weeks. Annual CT surveillance is needed after EVAR to ensure the stent-graft remains in position and there is no re-pressurisation of the aneurysm sac (endoleak).
Book an aortic aneurysm assessment in Delhi NCR at Yatharth Super Speciality Hospitals, Greater Noida. CT scans can be shared via WhatsApp for a pre-assessment.
Dr. Ved Prakash | Director CTVS — Yatharth Super Speciality Hospitals, Greater Noida
📞 +91-9355255106 |
Book Appointment →
