What Is Coronary Angiography? Procedure, Results and What Comes Next
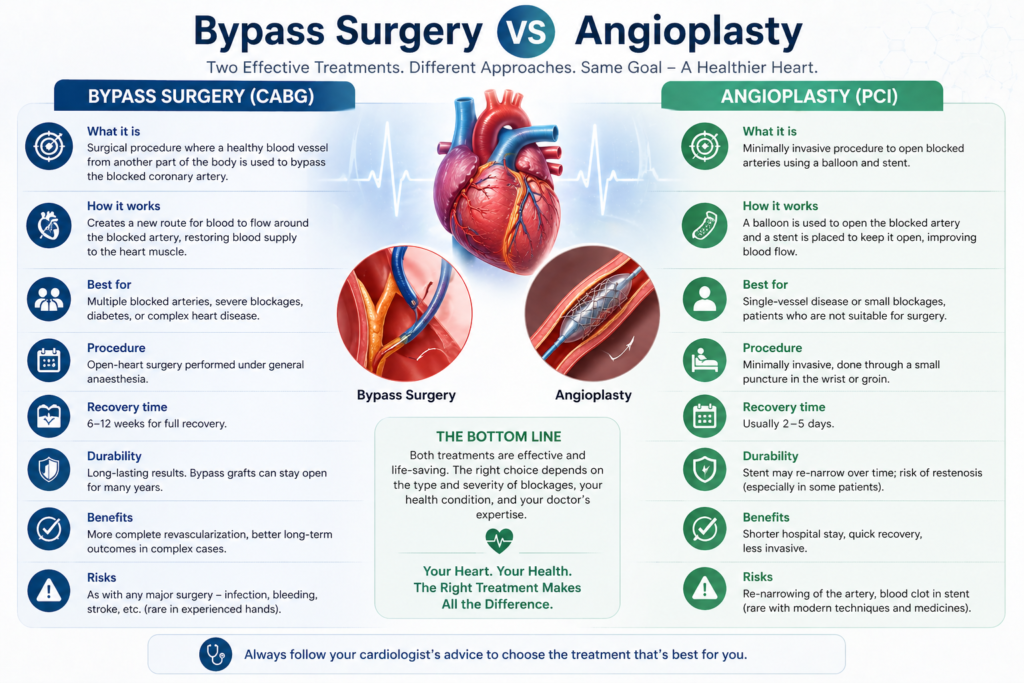
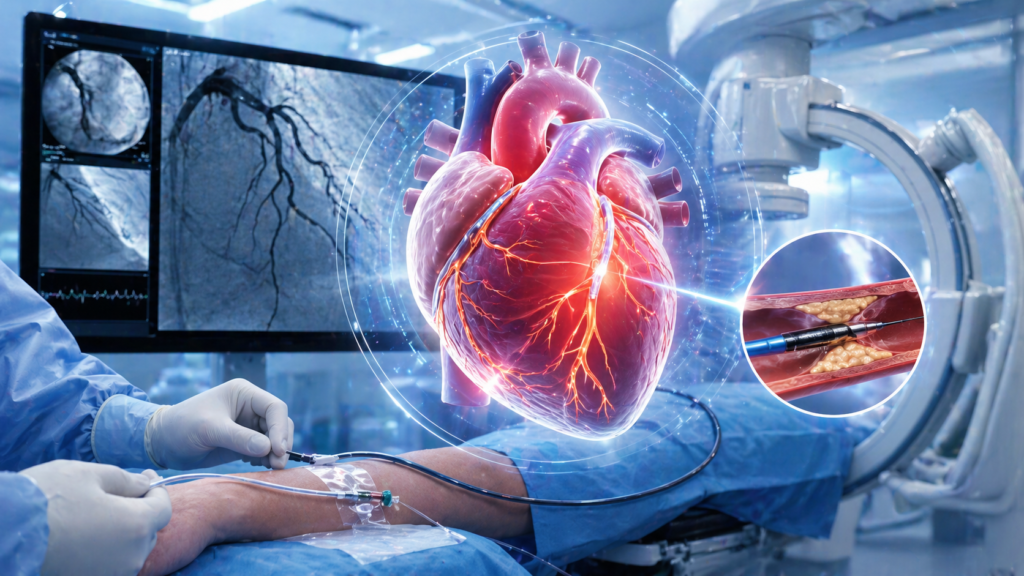
Coronary angiography is the gold-standard test for identifying blockages in the heart arteries — the investigation that gives your cardiologist or cardiac surgeon the road map they need to plan the right treatment. If you have been referred for coronary angiography, or if you already have an angiography report and want to understand what it means, Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, explains everything clearly. What Is Coronary Angiography? Coronary angiography is a catheter-based procedure that injects a special dye (contrast agent) directly into the coronary arteries while X-ray images are taken continuously. The dye makes the inside of the arteries visible on X-ray — revealing exactly where blockages are, how severe they are, and how many arteries are affected. Coronary angiography is performed in a cardiac catheterisation laboratory (cath lab), takes approximately 30–45 minutes, and is done under local anaesthesia — you are awake throughout. The catheter is most commonly inserted through the radial artery at the wrist (radial access) — which causes much less discomfort and allows you to go home the same day or the following morning. Why Is Coronary Angiography Recommended? Your cardiologist recommends coronary angiography when: You have chest pain on exertion that suggests angina An ECG, stress test (TMT), or echocardiogram shows changes suggesting blocked arteries You are being evaluated before major non-cardiac surgery (e.g., valve surgery) and are over 50 or have risk factors You have had a heart attack and require urgent assessment of the blocked artery CT coronary angiography has shown suspected significant blockages that need catheter-based confirmation What Happens During Coronary Angiography — Step by Step Preparation: You fast for 4–6 hours before the procedure. A thin tube (IV line) is placed in your arm. The access site (wrist or groin) is cleaned and numbed with local anaesthetic. Catheter insertion: A thin flexible tube (catheter) is inserted into the artery and guided up to the heart — guided by X-ray imaging. You feel pressure but no pain. Dye injection: Contrast dye is injected into each coronary artery. You briefly feel a warm flush through the chest — this lasts 10–15 seconds and is completely normal. Images recorded: X-ray images (cine-angiograms) are taken from multiple angles as the dye flows through the arteries — revealing any narrowings or blockages. Catheter removal: The catheter is removed and pressure applied to the access site. With radial (wrist) access, a compression band is placed and you can sit up and eat within an hour. How to Read Your Coronary Angiography Report This is the section no competitor explains — yet it is what every patient needs to understand. Percentage Blockage (Stenosis) 0–49% stenosis: Mild narrowing — does not significantly restrict blood flow. No intervention needed. Managed with medication and lifestyle changes. 50–69% stenosis: Moderate narrowing — may or may not be causing symptoms. Sometimes assessed further with an FFR (Fractional Flow Reserve) pressure wire to determine if it is truly restricting flow. 70–90% stenosis: Significant blockage — restricts blood flow. Almost always treated with angioplasty (stent) or included in a bypass surgery plan. 90–99% stenosis: Critical blockage — very high risk of heart attack. Urgent treatment required. 100% (total occlusion): Complete blockage — the artery is fully closed. Treatment depends on how long it has been blocked and whether viable heart muscle is at risk. Which Arteries Are Named in the Report LAD (Left Anterior Descending): Supplies the front of the heart — the most important coronary artery, also called the “widow maker” LCx (Left Circumflex): Supplies the side and back of the heart RCA (Right Coronary Artery): Supplies the right ventricle and back of the left ventricle Left Main: The trunk from which the LAD and LCx branch — a critical vessel; significant blockage here is a cardiac emergency What Happens After Coronary Angiography If a Blockage Is Found? Single, simple blockage in a non-diabetic patient: May be treated with angioplasty (stenting) immediately in the same session or scheduled shortly after Multiple blockages or complex anatomy: The coronary angiography images are reviewed by a Heart Team — cardiologist and cardiac surgeon — to decide between angioplasty and bypass surgery based on the SYNTAX score Left main disease: A cardiac surgery review is mandatory — bypass surgery is usually preferred No significant blockages: The angiography rules out coronary artery disease — your chest symptoms need evaluation for other causes If you have had coronary angiography and have been told surgery is needed, a cardiac second opinion in Delhi NCR from Dr. Ved Prakash gives you a complete, independent review of your angiogram images and a clear treatment recommendation. Share your angiography CD and report via WhatsApp. Frequently Asked Questions — What Is Coronary Angiography What is coronary angiography and is it dangerous? Coronary angiography is a catheter-based diagnostic procedure using dye and X-ray to reveal coronary artery blockages. It is extremely safe — the risk of serious complication is less than 0.1% in elective cases. It is performed under local anaesthesia and takes 30–45 minutes. What does 70% blockage on angiography mean? A 70% stenosis means the artery is narrowed to 30% of its normal diameter — significantly restricting blood flow. Most cardiologists and cardiac surgeons recommend treatment (angioplasty or bypass, depending on location) for blockages of 70% or more in major coronary arteries. Is coronary angiography painful? Not painful. The access site is numbed with local anaesthetic. Patients feel brief pressure when the catheter is moved, and a warm flush when the dye is injected — both normal and temporary. Most patients find coronary angiography significantly less uncomfortable than anticipated. What happens after coronary angiography if a blockage is found? A single simple blockage may be stented in the same session. Multiple or complex blockages are reviewed by a Heart Team who recommend angioplasty or bypass surgery based on the SYNTAX score and patient factors. Dr. Ved Prakash | Director CTVS — Yatharth Super Speciality Hospitals, Greater Noida 📞 +91-9355255106 | Bypass Surgery Consultation