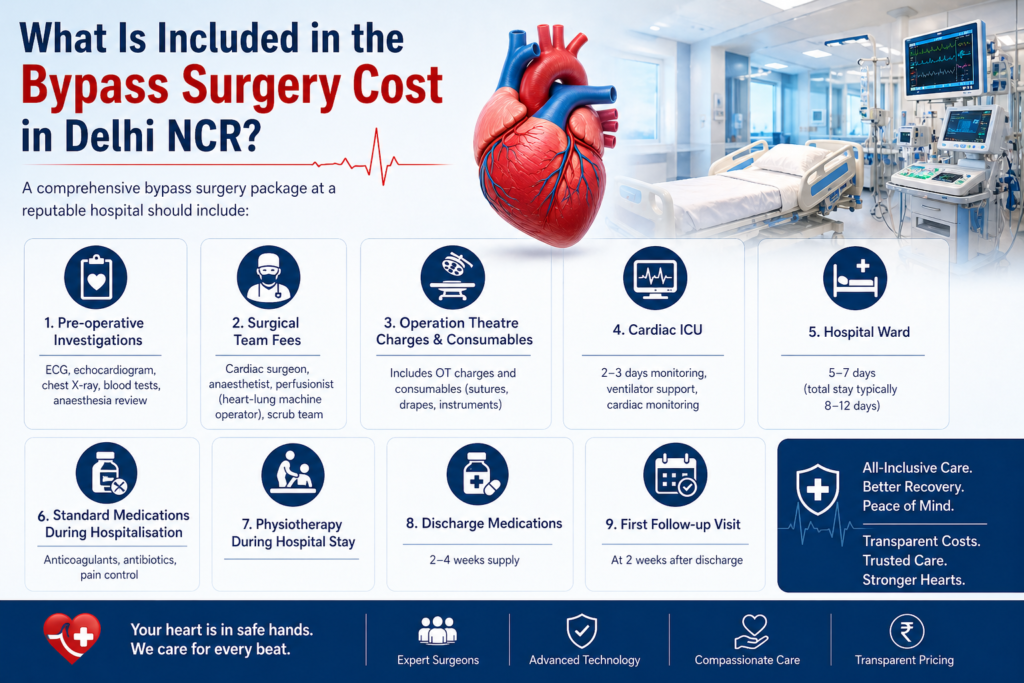
Bypass surgery cost in Delhi NCR is the first question most families ask after an angiogram shows significant blockages — and getting a clear, honest answer is harder than it should be. This guide from Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, gives you the complete picture: what bypass surgery cost in Delhi NCR covers, what affects the final bill, how insurance and government schemes work, and what you can do to ensure you receive the best care at the right price. Bypass Surgery Cost in Delhi NCR — 2026 Price Ranges Bypass surgery cost in Delhi NCR varies based on the hospital category, room type, number of bypass grafts, and patient complexity. As a general guide for 2026: Hospital Category Shared Ward Semi-Private Room Private Room Government hospital (AIIMS, Safdarjung) ₹80,000–1,50,000 ₹1,50,000–2,50,000 ₹2,50,000–3,50,000 Mid-tier private hospital (Yatharth, Sarvodaya, BLK) ₹2,50,000–3,50,000 ₹3,50,000–4,50,000 ₹4,50,000–5,50,000 Premium hospital (Apollo, Max, Fortis Escorts) ₹4,00,000–5,50,000 ₹5,50,000–7,00,000 ₹7,00,000–9,00,000 Note: These are indicative ranges for 2026. Bypass surgery cost in Delhi NCR varies based on individual patient factors — actual quotes should be obtained from the hospital’s billing department after clinical assessment. What Is Included in the Bypass Surgery Cost in Delhi NCR? A comprehensive bypass surgery package at a reputable hospital should include: Pre-operative investigations: ECG, echocardiogram, chest X-ray, blood tests, anaesthesia review Surgical team fees: cardiac surgeon, anaesthetist, perfusionist (heart-lung machine operator), scrub team Operation theatre charges and consumables (sutures, drapes, instruments) Cardiac ICU: 2–3 days monitoring, ventilator support, cardiac monitoring Hospital ward: 5–7 days (total stay typically 8–12 days) Standard medications during hospitalisation: anticoagulants, antibiotics, pain control Physiotherapy during hospital stay Discharge medications: 2–4 weeks supply First follow-up visit at 2 weeks What is often NOT included in the quoted package: coronary angiography before surgery (₹15,000–30,000 separately), CT angiography if needed, blood products if transfusion required, complications or prolonged ICU stay beyond the package duration, and outpatient medications after the first prescription. Factors That Affect Bypass Surgery Cost in Delhi NCR Number of bypass grafts: Single bypass costs less than triple bypass — more grafts mean longer operative time and more graft material On-pump vs off-pump: Off-pump (OPCAB) surgery typically adds 10–15% to the cost due to the specialised stabiliser equipment Arterial grafts used: Total arterial revascularisation (LIMA + radial artery) may add to cost but improves long-term durability Patient complexity: Emergency surgery, redo bypass (after previous surgery), low ejection fraction, or concurrent valve surgery — all increase cost ICU duration: Patients with complications who stay in ICU longer than the package duration incur additional daily ICU charges (₹8,000–20,000/day depending on hospital) Room category: The single largest variable in bypass surgery cost in Delhi NCR — private room vs shared ward can differ by ₹50,000–1,00,000 for the same surgery Insurance Coverage for Bypass Surgery Cost in Delhi NCR Most comprehensive health insurance policies cover bypass surgery cost in Delhi NCR as an inpatient procedure. Key points: Cashless treatment: Available at empanelled hospitals. Submit pre-authorisation to your TPA (Third Party Administrator) 2–3 days before elective surgery with the angiogram report and surgeon’s recommendation letter. Most private hospitals including Yatharth Hospital have dedicated insurance facilitation teams. Waiting period: Most policies have a 1–4 year waiting period for pre-existing conditions. If bypass surgery is needed urgently (within the waiting period), claim reimbursement after hospital discharge — insurers cannot deny medically necessary emergency surgery. Sub-limits: Some older policies have sub-limits on ICU charges or surgeon fees — check your policy schedule before finalising the hospital. Top-up policies: If your current sum insured is below ₹5 lakhs and bypass surgery cost in Delhi NCR exceeds this, a top-up policy bridges the gap — worth considering for every cardiac patient. Government Schemes Covering Bypass Surgery Cost in Delhi NCR Ayushman Bharat PM-JAY: Covers bypass surgery cost in Delhi NCR up to ₹5 lakhs per family per year for eligible beneficiaries (below poverty line / specific government categories). Yatharth Hospital is empanelled. Check eligibility at pmjay.gov.in. CGHS (Central Government Health Scheme): Covers central government employees and pensioners. Bypass surgery cost in Delhi NCR is reimbursed at CGHS package rates — which may be lower than private rates. Empanelment status of hospital matters. ECHS (Ex-Servicemen Contributory Health Scheme): Similar to CGHS for defence personnel. Yatharth Hospital Greater Noida accepts ECHS cards. State government schemes: UP government’s Mukhyamantri Jan Arogya Yojana covers eligible UP residents for bypass surgery cost at empanelled hospitals in Greater Noida. How to Reduce Bypass Surgery Cost in Delhi NCR Legitimately Choose a shared ward or semi-private room — the surgery is identical, only the room differs Ask for a detailed package quote in writing before admission — including what extras will be charged Ensure pre-authorisation is obtained from your insurer before the surgery date Do not delay surgery while financial arrangements are made — deterioration may convert an elective surgery to an emergency, significantly increasing cost and risk Ask specifically whether the surgeon who quoted your case will personally perform your surgery Bypass Surgery Cost at Yatharth Super Speciality Hospitals, Greater Noida Bypass surgery cost in Delhi NCR at Yatharth Super Speciality Hospitals, Greater Noida is in the mid-tier range — offering the surgical expertise of Dr. Ved Prakash (8+ years experience including Medanta, Narayana, and Sarvodaya) in a NABH-accredited hospital at a price point accessible to UP and Delhi NCR patients without requiring travel to central Delhi. Cashless insurance, Ayushman Bharat, CGHS, ECHS, and corporate tie-ups are available. For a specific quote for your case, share your angiogram report via WhatsApp or book a bypass surgery consultation in Delhi NCR. Frequently Asked Questions — Bypass Surgery Cost in Delhi NCR What is the average bypass surgery cost in Delhi NCR in 2026? The average bypass surgery cost in Delhi NCR in 2026 is ₹3,50,000–4,50,000 in a semi-private room at a reputable mid-tier private hospital. At premium hospitals (Apollo, Max, Fortis), bypass surgery cost in Delhi NCR ranges ₹5,50,000–8,00,000 for comparable surgery in a private room. Is bypass surgery cost