The bypass surgery vs angioplasty decision is the most important — and most frequently misunderstood — choice in cardiac treatment. Both procedures treat blocked coronary arteries. Both save lives. But choosing the wrong one for your anatomy can mean going back for another procedure in 5 years — or worse. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, explains exactly how bypass surgery vs angioplasty is evaluated — and what determines the right answer for each patient.
Bypass Surgery vs Angioplasty — What Each Procedure Does
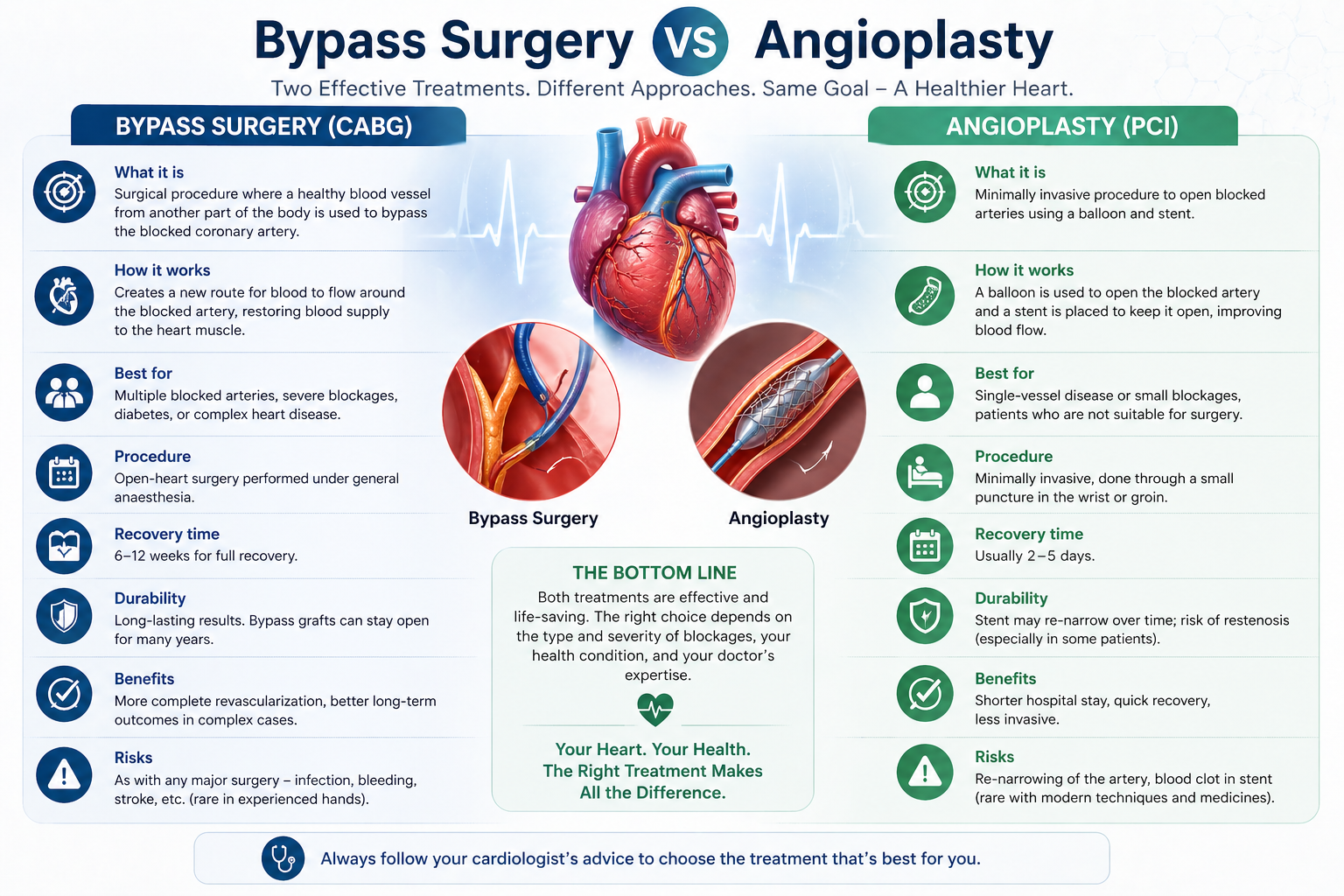
Before comparing bypass surgery vs angioplasty, the basic mechanism of each must be clear.
Angioplasty (PCI / stenting): A thin catheter is inserted through the wrist or groin artery and guided to the blockage. A balloon inflates to widen the artery, and a metal mesh tube (stent) is left in place to keep it open. No chest incision. Recovery in 1–3 days. Best for: a single blockage or a simple two-vessel disease in a non-diabetic patient.
Bypass surgery (CABG): A healthy blood vessel is taken from the chest wall or leg and sewn in to bypass the blocked section entirely — creating a permanent new route for blood. Requires a chest incision and 7–10 days in hospital. Best for: multiple blockages, left main disease, diabetes, or complex anatomy that stents cannot address durably.
The Clinical Criteria Used to Choose Between Bypass Surgery vs Angioplasty
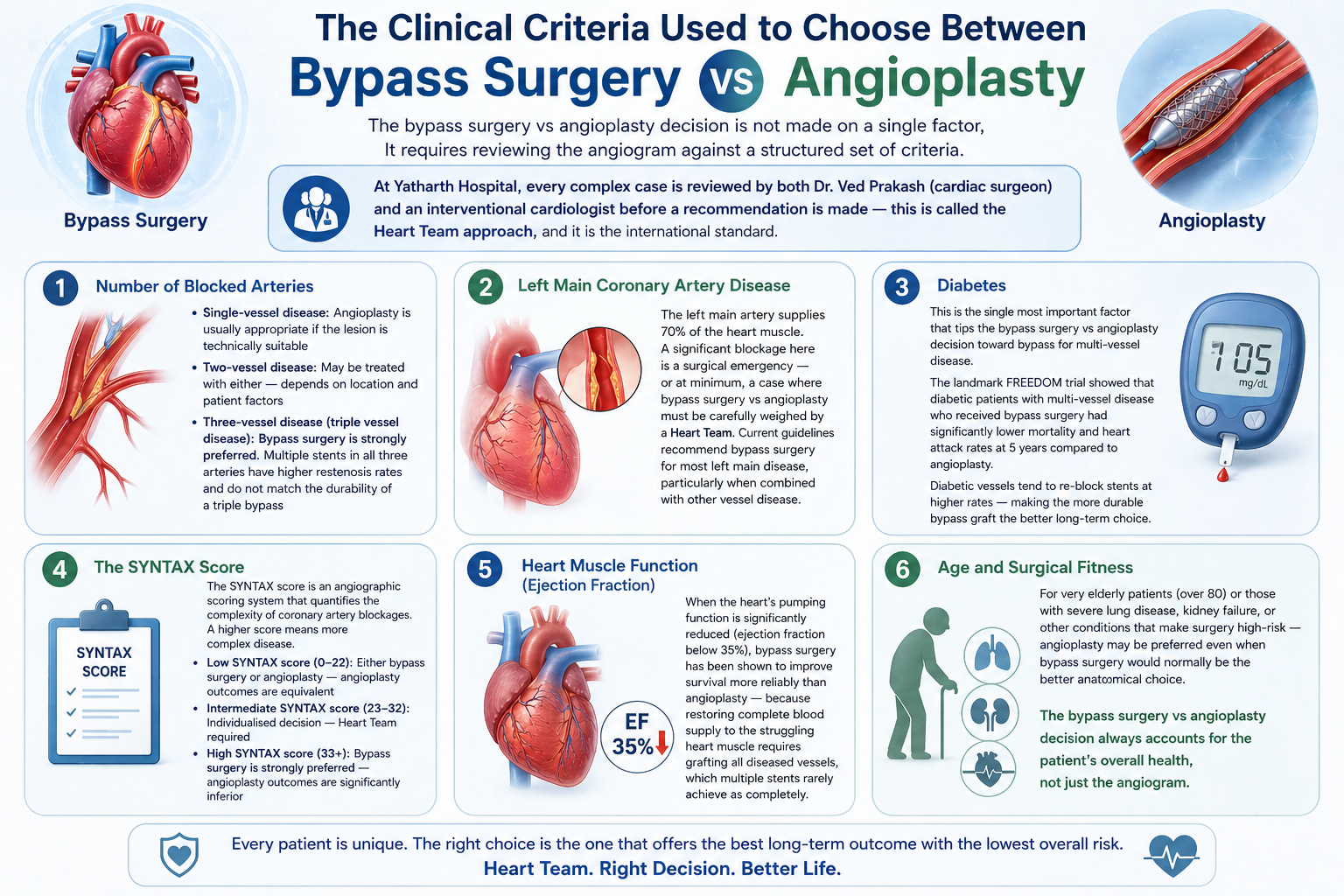
The bypass surgery vs angioplasty decision is not made on a single factor. It requires reviewing the angiogram against a structured set of criteria. At Yatharth Hospital, every complex case is reviewed by both Dr. Ved Prakash (cardiac surgeon) and an interventional cardiologist before a recommendation is made — this is called the Heart Team approach, and it is the international standard.
1. Number of Blocked Arteries
- Single-vessel disease: Angioplasty is usually appropriate if the lesion is technically suitable
- Two-vessel disease: May be treated with either — depends on location and patient factors
- Three-vessel disease (triple vessel disease): Bypass surgery vs angioplasty — bypass surgery is strongly preferred. Multiple stents in all three arteries have higher restenosis rates and do not match the durability of a triple bypass
2. Left Main Coronary Artery Disease
The left main artery supplies 70% of the heart muscle. A significant blockage here is a surgical emergency — or at minimum, a case where bypass surgery vs angioplasty must be carefully weighed by a Heart Team. Current guidelines recommend bypass surgery for most left main disease, particularly when combined with other vessel disease.
3. Diabetes
This is the single most important factor that tips the bypass surgery vs angioplasty decision toward bypass for multi-vessel disease. The landmark FREEDOM trial showed that diabetic patients with multi-vessel disease who received bypass surgery had significantly lower mortality and heart attack rates at 5 years compared to angioplasty. Diabetic vessels tend to re-block stents at higher rates — making the more durable bypass graft the better long-term choice.
4. The SYNTAX Score
The SYNTAX score is an angiographic scoring system that quantifies the complexity of coronary artery blockages. A higher score means more complex disease. In general:
- Low SYNTAX score (0–22): Either bypass surgery or angioplasty — angioplasty outcomes are equivalent
- Intermediate SYNTAX score (23–32): Individualised decision — Heart Team required
- High SYNTAX score (33+): Bypass surgery is strongly preferred — angioplasty outcomes are significantly inferior
5. Heart Muscle Function (Ejection Fraction)
When the heart’s pumping function is significantly reduced (ejection fraction below 35%), bypass surgery has been shown to improve survival more reliably than angioplasty — because restoring complete blood supply to the struggling heart muscle requires grafting all diseased vessels, which multiple stents rarely achieve as completely.
6. Age and Surgical Fitness
For very elderly patients (over 80) or those with severe lung disease, kidney failure, or other conditions that make surgery high-risk — angioplasty may be preferred even when bypass surgery would normally be the better anatomical choice. The bypass surgery vs angioplasty decision always accounts for the patient’s overall health, not just the angiogram.
Bypass Surgery vs Angioplasty — Side-by-Side Comparison
| Factor | Bypass Surgery (CABG) | Angioplasty (PCI) |
| Recovery time | 6–12 weeks | 1–3 days |
| Best for diabetes + multi-vessel | Yes — strongly preferred | Higher restenosis risk |
| Left main disease | Preferred in most cases | Only in selected anatomy |
| Graft / stent durability | LIMA graft: 15–20+ years | Drug-eluting stent: 10–15 years |
| Three-vessel disease | Strongly preferred | High SYNTAX score → inferior outcomes |
| Blood thinners needed | Aspirin only (lifelong) | Aspirin + Clopidogrel (12 months minimum) |
| Can be repeated if it fails | Yes, but higher risk redo | Yes, repeat angioplasty or bypass |
When Bypass Surgery vs Angioplasty Is Not Clear-Cut — Get a Second Opinion
If your cardiologist has recommended angioplasty for multi-vessel disease and you are diabetic — or if you have been offered bypass surgery and want to understand whether angioplasty is viable — a cardiac second opinion in Delhi NCR from a CTVS surgeon who reviews your angiogram independently is the most important step before making a decision. Share your angiogram CD and report via WhatsApp with Dr. Ved Prakash for a pre-assessment.
Frequently Asked Questions — Bypass Surgery vs Angioplasty
Is bypass surgery vs angioplasty always a surgeon’s decision?
No — the decision should be made jointly by an interventional cardiologist and a cardiac surgeon reviewing the angiogram together. A Heart Team approach using the SYNTAX score is the international standard. Any patient offered one option without this joint review should ask why.
Which is better — bypass surgery or angioplasty?
For single, simple blockages in otherwise healthy patients — angioplasty is usually sufficient. For three-vessel disease, left main disease, or diabetic patients with multiple blockages — bypass surgery gives more durable long-term results. There is no universal winner; the anatomy of the blockages decides.
Can bypass surgery be done after failed angioplasty?
Yes — bypass surgery is commonly performed after a stent fails (restenosis) or when multiple stents have been placed and further angioplasty is no longer feasible. It is technically more demanding in these cases but still delivers excellent results at experienced centres.
How long do stents last compared to bypass grafts?
Modern drug-eluting stents last 10–15 years in most patients. The LIMA arterial bypass graft lasts 15–20+ years and remains open in over 90% of patients at 10 years. This durability difference is one of the main reasons bypass is preferred for younger patients and those with multiple blockages.
Dr. Ved Prakash | Director CTVS — Yatharth Super Speciality Hospitals, Greater Noida
📞 +91-9355255106 |
Bypass Surgery Consultation →
