 What Parents Need to Know After a TOF Diagnosis: Tetralogy of Fallot — TOF — is the most common cyanotic congenital heart defect, and a diagnosis that most parents receive with no preparation and very little information about what comes next. If your baby has just been diagnosed with TOF, this guide explains what it means, what symptoms to watch for at home, what surgery involves, and — critically — what your child’s life looks like after repair. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, has performed TOF repairs from early infancy across Medanta, Narayana, and Yatharth Hospital.
What Parents Need to Know After a TOF Diagnosis: Tetralogy of Fallot — TOF — is the most common cyanotic congenital heart defect, and a diagnosis that most parents receive with no preparation and very little information about what comes next. If your baby has just been diagnosed with TOF, this guide explains what it means, what symptoms to watch for at home, what surgery involves, and — critically — what your child’s life looks like after repair. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, has performed TOF repairs from early infancy across Medanta, Narayana, and Yatharth Hospital.
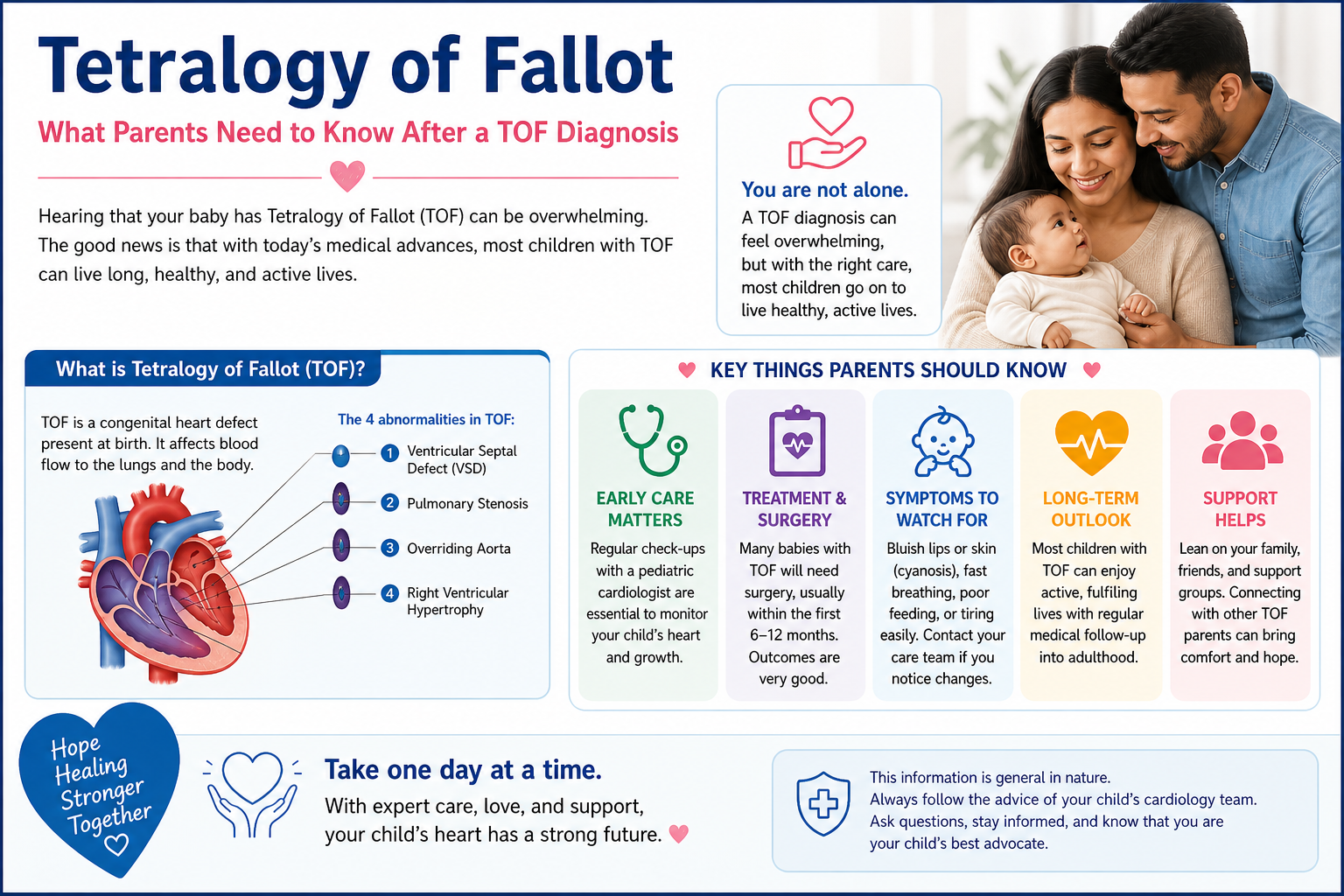
What Is Tetralogy of Fallot?
Tetralogy of Fallot is four structural abnormalities that occur together in the same heart. Understanding all four is important because they interact — each one making the others worse:
- A large VSD (ventricular septal defect) — a large hole between the two lower chambers, allowing blue (deoxygenated) blood to mix with red (oxygenated) blood.
- Pulmonary stenosis — narrowing of the outflow from the right ventricle to the lungs. This obstruction means less blood reaches the lungs to pick up oxygen, and more blue blood is pushed through the VSD to the body instead.
- Overriding aorta — the aorta sits directly over the VSD rather than exclusively over the left ventricle, receiving a mix of blue and red blood from both chambers.
- Right ventricular hypertrophy — the right ventricle thickens because it is pumping against the obstructed pulmonary outflow. This worsens over time if repair is delayed.
The net result: the body continuously receives blood that has not been fully oxygenated — causing the characteristic blue discolouration (cyanosis) of Tetralogy of Fallot.
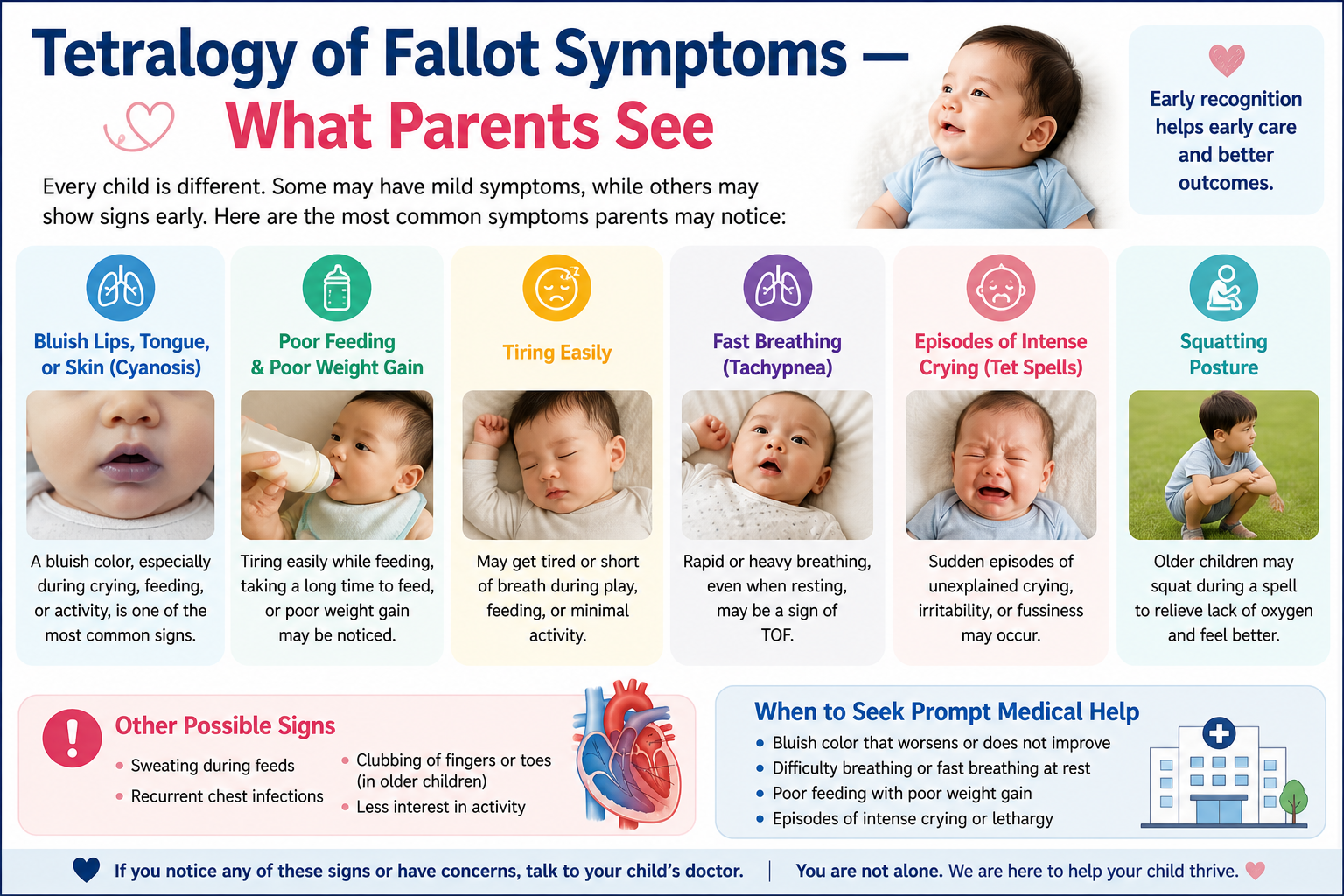
Tetralogy of Fallot Symptoms — What Parents See
Cyanosis — The Blue Baby Appearance
Blue or purple discolouration of the lips, tongue, fingernails, and toenails. In some babies with TOF, cyanosis is obvious at birth. In others — particularly where the pulmonary stenosis is mild — cyanosis develops gradually in the first weeks of life as the ductus arteriosus (a foetal blood vessel that keeps oxygen supply adequate in the womb) closes after birth. A baby who was pink at birth and becomes increasingly blue in the first month needs urgent cardiac assessment.
Tet Spells — The Most Frightening Symptom
A tet spell is a hypercyanotic episode — a sudden, dramatic worsening of cyanosis triggered by anything that decreases pulmonary blood flow: crying, feeding, defecation, waking from sleep, or even nothing obvious. During a tet spell the baby turns intensely blue, becomes extremely distressed and inconsolable, breathes very fast, and may go limp or briefly lose consciousness from cerebral hypoxia.
Tet spells are caused by spasm of the right ventricular outflow tract — the already-narrowed channel from the right ventricle to the lungs temporarily clamps shut, redirecting almost all right-sided output through the VSD to the body. Almost no blood reaches the lungs. Oxygen saturation plummets.
If your baby has a tet spell: pull the knees firmly up to the chest (squatting position for an infant), keep the baby calm, and call emergency services immediately. Tet spells require hospital assessment and accelerate the need for surgery. Do not wait to see if it settles.
Squatting in Older Unrepaired Children
Older children with unrepaired or partially palliated TOF instinctively squat after physical activity. Squatting compresses the femoral arteries — increasing systemic vascular resistance and reducing the right-to-left shunt through the VSD — temporarily pushing more blood to the lungs and relieving cyanosis. It is one of the most specific clinical signs in all of paediatric cardiology.
Other Signs
- Poor growth and weight gain — the body cannot support normal growth when oxygen delivery is chronically reduced
- Exercise intolerance in older unrepaired children — breathlessness and cyanosis with minimal exertion
- Clubbing of fingers and toes — develops after months of chronic cyanosis
How Tetralogy of Fallot Is Diagnosed
- Foetal echocardiogram: TOF is detectable at the 18–20 week anomaly scan in many cases — allowing planned delivery at a centre with paediatric cardiac surgery capability.
- Neonatal echocardiogram: Confirms the anatomy — size of the VSD, degree of pulmonary stenosis, position of the aorta, and right ventricular size.
- Pulse oximetry screening: Low oxygen saturation detected on routine newborn screening triggers further investigation.
- CT cardiac angiography: Used before surgery when the pulmonary artery anatomy needs detailed 3D mapping — particularly important for the branch pulmonary arteries which can be hypoplastic in severe TOF.
Tetralogy of Fallot Surgery — What Is Done
Complete surgical repair of TOF is performed under general anaesthesia and cardiopulmonary bypass. The operation addresses all the abnormalities simultaneously:
- VSD closure: The hole between the ventricles is closed with a patch — stopping the mixing of blue and red blood completely.
- Relief of pulmonary stenosis: The narrowed right ventricular outflow tract is widened by resecting obstructing muscle bundles, and often by placing a patch across the outflow tract or pulmonary valve to enlarge it. If the pulmonary valve itself is severely abnormal it may be removed — leaving the outflow tract open (transannular patch). This effectively relieves obstruction but results in pulmonary regurgitation.
- Result: Blue blood now goes through the pulmonary artery to the lungs normally. Oxygenated blood returns and goes through the aorta to the body. Cyanosis resolves.
Surgery is typically performed between 3 and 6 months of age. If tet spells are occurring before this age, surgery is brought forward without delay. Results at experienced centres: operative mortality below 2–3%, complete repair achieved in virtually all cases.
Life After TOF Surgery — The Honest Picture
This is what parents most need to understand — and what most articles do not explain.
The good news: The vast majority of children repaired in infancy grow up completely normally. They attend mainstream school, participate in sport, develop normally in every way. Most go on to live independent adult lives — working, driving, having children of their own.
What requires lifelong monitoring:
- Annual echocardiogram — monitoring right ventricular size and function over time
- Pulmonary regurgitation — when the pulmonary valve was enlarged or removed during repair, the resulting leakage causes the right ventricle to gradually enlarge over years. This is well tolerated through childhood and adolescence but needs monitoring.
- Pulmonary valve replacement in adulthood: Approximately 25–30% of TOF patients require a pulmonary valve replacement — surgical or catheter-based (PPVI) — typically between ages 20 and 35, when the right ventricle has enlarged to a threshold that warrants intervention. This is a planned, elective, non-emergency procedure — not a crisis. Parents should know about it from early on so it is not a shock when the cardiologist raises it in adulthood.
For more on the range of congenital heart defects treated in children including VSD in babies, visit the paediatric cardiac surgery blog. To consult Dr. Ved Prakash about a TOF diagnosis, share echocardiogram and CT reports via WhatsApp for a pre-assessment before attending paediatric heart surgery clinic at Yatharth Hospital.
Frequently Asked Questions — Tetralogy of Fallot Symptoms Treatment
What is a tet spell and what should I do if my baby has one?
A tet spell is a sudden, severe episode of cyanosis caused by spasm of the right ventricular outflow tract. The baby turns intensely blue and becomes very distressed. Immediately place the baby in a knee-chest position, keep them calm, and call emergency services. Tet spells require urgent hospital assessment and accelerate the need for surgery.
What are the symptoms of Tetralogy of Fallot in a newborn?
Cyanosis — blue or purple discolouration of the lips, tongue, and nails. May be present at birth or develop in the first weeks as the ductus arteriosus closes. Low oxygen saturation on routine screening and a murmur on examination lead to the diagnosis.
At what age is Tetralogy of Fallot surgery performed?
Typically between 3 and 6 months of age. Earlier if tet spells are occurring. Not delayed beyond 6 months at experienced centres — sustained right ventricular pressure overload causes irreversible muscle damage if repair is too long deferred.
What is the long-term outlook after Tetralogy of Fallot surgery?
Most children live completely normal lives after repair. 25-year survival rates exceed 94%. Lifelong cardiology follow-up is needed. Approximately 25–30% will need a pulmonary valve replacement in adulthood — a planned elective procedure, not an emergency.
Dr. Ved Prakash | Director, CTVS — Yatharth Super Speciality Hospitals, Greater Noida
📞 +91-9355255106 |
📧 drvedprakash@gmail.com |
Book Appointment →