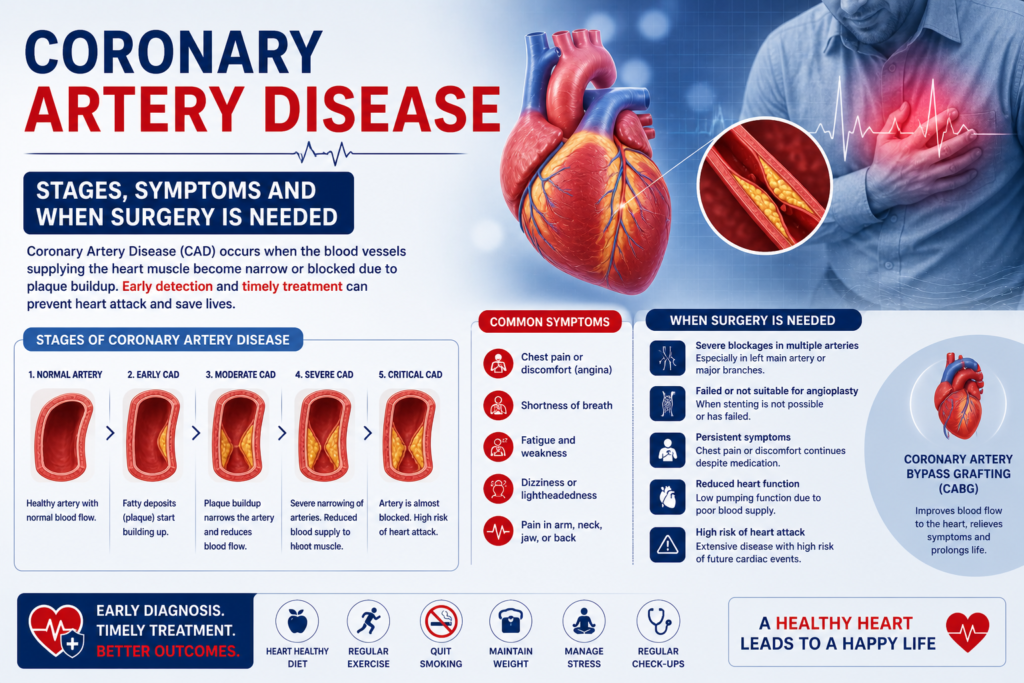
Coronary Artery Disease — Stages, Symptoms and When Surgery Is Needed
Coronary artery disease is not a single event — it is a decades-long process that progresses through identifiable stages, with each stage carrying different symptoms, different risks, and different treatment implications. Understanding where you or a family member sits in this progression is the most important step toward making the right treatment decision. Dr. Ved Prakash, Director of CTVS at Yatharth Super Speciality Hospitals, Greater Noida, explains coronary artery disease stages and symptoms, and when each stage crosses the threshold for surgical intervention. What Is Coronary Artery Disease? Coronary artery disease (CAD) is the buildup of atherosclerotic plaque — a mixture of cholesterol, inflammatory cells, calcium, and fibrous tissue — inside the walls of the coronary arteries that supply the heart muscle with blood. As this plaque accumulates over years, it progressively narrows the artery lumen. When narrowing reaches approximately 70%, blood flow during exertion is insufficient and symptoms begin. When a plaque ruptures and a clot forms suddenly, the result is a heart attack. India has one of the highest burdens of coronary artery disease globally — affecting patients 10–15 years younger on average than in Western countries, and with a disproportionately high rate of multi-vessel disease at first presentation. Coronary Artery Disease Stages — The Full Progression Stage 1 — Subclinical Atherosclerosis (No Symptoms) Plaque begins accumulating in the coronary artery walls from as early as the 20s and 30s in high-risk individuals — those with diabetes, hypertension, high cholesterol, a strong family history, or heavy smoking history. At this stage, the narrowing is less than 50% and blood flow is not restricted. There are no symptoms whatsoever. This stage is detectable with CT coronary calcium scoring and CT coronary angiography — tests that show plaque burden before any symptoms develop. This is the stage where lifestyle modification and statin therapy are most effective at slowing or halting progression. Stage 2 — Stable Angina (Predictable Chest Pain on Exertion) When the coronary artery narrows beyond 70%, blood flow during physical exertion becomes insufficient for the heart muscle’s increased demand. The result is stable angina — chest pain or tightness that comes on predictably after a certain amount of exertion and resolves completely within 5–10 minutes of rest. Patients describe stable angina as: central chest tightness, pressure, heaviness, or aching — sometimes radiating to the left arm, jaw, or between the shoulder blades. The pain is consistent — the same exertion produces the same symptoms. It does not occur at rest. If you develop this symptom pattern, see a cardiologist immediately for an ECG, stress test, and likely coronary angiography. Diabetic patients and women frequently do not experience typical chest pain — they present with breathlessness, jaw pain, left arm pain, or unexplained fatigue as their angina equivalent. These atypical presentations lead to delayed diagnosis. Stage 3 — Unstable Angina / NSTEMI (Plaque Rupture) When atherosclerotic plaque becomes unstable — thin-capped, inflamed, and vulnerable — it can rupture. A ruptured plaque triggers immediate clot formation (thrombus) at the rupture site. If the clot partially blocks the artery, blood flow at rest is compromised. The result is: Unstable angina: Chest pain at rest, or with minimal exertion, or that is getting progressively more frequent and severe. A dangerous change from a previously stable pattern. NSTEMI (Non-ST Elevation Myocardial Infarction): Partial blockage with some heart muscle damage — troponin rises on blood tests but the ECG does not show the classic ST elevation of a full heart attack. Both unstable angina and NSTEMI require hospital admission and urgent coronary angiography — typically within 24–48 hours. This is not a situation where a patient should wait for a scheduled appointment. Stage 4 — STEMI (Complete Heart Attack) When the clot at the rupture site completely occludes the artery, blood supply to the downstream heart muscle stops entirely. This is a STEMI — ST-Elevation Myocardial Infarction — a full heart attack. Every minute of complete occlusion destroys heart muscle that will never recover. Time from symptom onset to opening the blocked artery is the single most important determinant of how much heart muscle is saved. STEMI symptoms: Sudden severe chest pain at rest — crushing, squeezing, or pressure sensation. May radiate to the left arm, jaw, or back. Often accompanied by sweating, nausea, breathlessness, and a feeling of impending doom. Can also present without chest pain in diabetics — only breathlessness and sweating. STEMI is a medical emergency. Call emergency services immediately. Do not drive yourself to hospital. How Many Arteries Are Blocked — And Why It Matters Coronary artery disease is classified by how many vessels are affected: Vessel Count Definition Typical Treatment Single vessel One artery with significant blockage Angioplasty usually appropriate Two vessel (double vessel) Two arteries significantly blocked Heart Team decision — depends on location and patient profile Three vessel (triple vessel) All three main arteries blocked Bypass surgery strongly preferred Left main disease Trunk artery before LAD and LCx Bypass surgery in most cases Risk Factors That Accelerate Coronary Artery Disease Diabetes — the single most aggressive accelerator of CAD in Indian patients. Doubles the risk and significantly worsens outcomes after heart attack. Hypertension — damages the arterial endothelium, accelerating plaque deposition Smoking — directly toxic to coronary endothelium; smokers develop CAD 10 years earlier than non-smokers High LDL cholesterol — primary driver of plaque accumulation; statin therapy is the cornerstone of prevention Family history — first-degree relative with heart disease before 55 (men) or 65 (women) doubles your risk Sedentary lifestyle and central obesity — particularly the android fat distribution pattern common in South Asians When Coronary Artery Disease Requires Surgery Not all coronary artery disease requires surgery. The threshold is determined by: Symptoms that are not adequately controlled with medication Anatomical findings on angiography that predict a survival benefit from surgery — triple vessel disease, left main disease, or high SYNTAX score Ejection fraction below 35% with multi-vessel disease — where complete revascularisation by surgery improves both symptoms and survival The decision between bypass